These are some associated notes and references for a talk I gave at EuSEM 2019 in Prague.
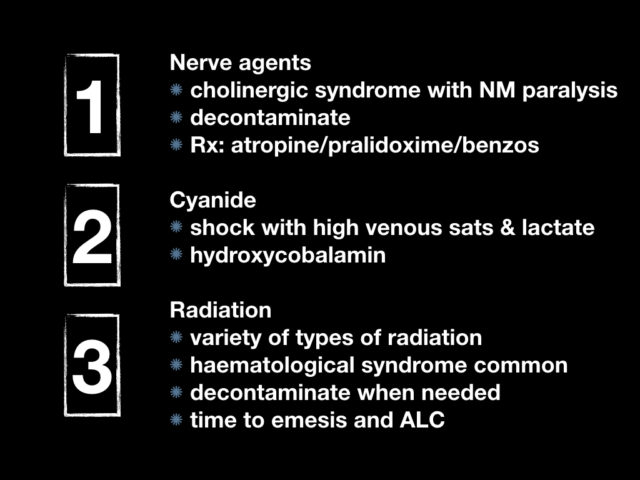
Part 1

this was the murder of Kim Jong Nam in Kuala Lumpur international airport on February 13th 2017. He was the older step brother of the current North Korean leader, Kim Jong Un. They were raised separately and apparently had never met. Kim Jong Nam was for many years expected to be the next leader of North Korea after his father died. However he fell out of favour and was exiled from North Korea. His younger brother had tried to assassinate him on several occasions prior to this.
The malaysian authorities reported that Kim was killed with the nerve agent VX. VX stands for “venomous agent X” and is probably the most well known of the V series agents. In British spy code it was known as purple possum. The V series of agents were developed as most of these were as a pesticide by a British firm in 1952. Once they realised how toxic it was, it was quickly snapped up by places like Porton Down in the UK and in the early 60s large amounts of VX were stockpiled by the US. In the case of Kim Jong Nam it is suspected that it was used as a binary agent where two chemical compounds only become VX when combined at the time of administration – thus making it easier to transport and safer for the person administering the poison
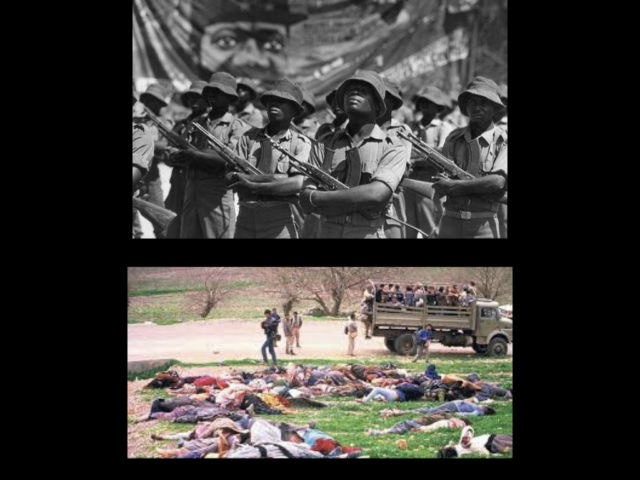
VX was reportedly used by Cuba in its role in the Angolan civil in 1984 was and was used by Sadaam Hussein in the Halabja attacks agains the the Kurds in northern Iraq in 1988.

while not VX, nerve agents have been used in the in the western world as part of a terrorist intervention such as the 1995 sarin gas attacks or more recently the poisoning of the Skirpals in salisbury in the UK

VX has its action at the NMJ. Contained in the little vesicles marked 3 is all the goodness of Ach. Following the arrival of a depolarisation down the nerve the vesicles release Ach into the junction. Ach binds with 4, the nicotinic receptor, and like a sequence of dominos falling a sequence is kicked off resulting in muscular contraction.
the muscarinic Ach receptors exist where nerves meet smooth muscles and glands. There are also Ach receptors in the brain.
Acetylcholinesterase exists in large amounts in the cleft of the NMJ. it’s role is to break down Ach to prevent ongoing stimulation of the receptor.
VX inhibits acetylcholinesterase so all of a sudden the Ach binding sites are activated and not being deactivated as they should be.
This has a number of effects as follows
Muscarinic
massive respiratory secretions, bronchospasm, severe diaphoresis, vomiting, diarrhea, meiosis, lacrimation
Nicotinic
voluntary muscle fasciculation and spasm, followed by fatigue and flaccidity
Central
seizures, central apnea
ED Management
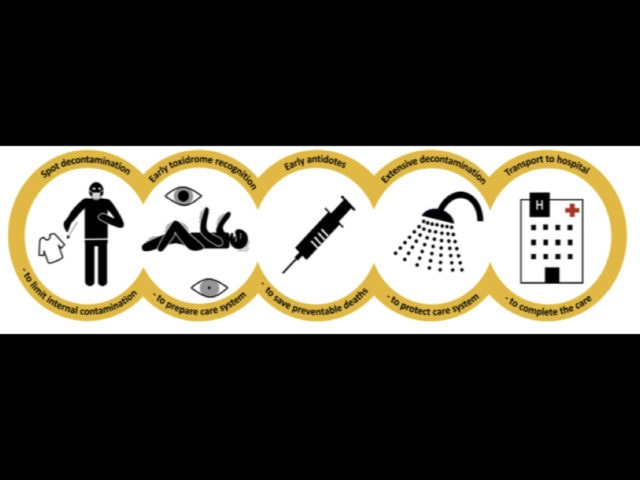
the CBRN chain of survival was recently published in 2019 by the paris fire brigade and is an excellent illustration of the response. Initial decontamination is wiping with paper roll and disrobing. this is likely 80% of decontamination
Atropine will be used to dry up the patient and reverse the tachycardia. Pralidoxime will help combat the nicotinic effects (muscular paralysis) , Pralidoxime can help resurrect the inhibited AChE, hopefully enough to enable muscular contraction. And benzos are used to manage the frequent presence of seizures
References:
Hulse EJ, Haslam JD, Emmett SR, Woolley T. Organophosphorus nerve agent poisoning: managing the poisoned patient. Br J Anaesth. Elsevier Ltd; 2019 Jun 24;123(4):1–7.
Allister VJ, C MT, L MR. Novichok: a murderous nerve agent attack in the UK. Clinical Toxicology. Informa UK Limited, trading as Taylor & Francis Group; 2018 Sep 17;0(0):1–5.
Chai PR, Hayes BD, Erickson TB, Boyer EW. Novichok agents: a historical, current, and toxicological perspective. Toxicol Commun. 2nd ed. 2018;2(1):45–8.
Calamai F, Derkenne C, Jost D, Travers S, Klein I, Bertho K, et al. The chemical, biological, radiological and nuclear (CBRN) chain of survival: a new pragmatic and didactic tool used by Paris Fire Brigade. Critical Care; 2019 Feb 20;:1–3.
Okumura T, Suzuki K, Fukuda A, Kohama A, Takasu N, Ishimatsu S, et al. The Tokyo subway sarin attack: disaster management, Part 2: Hospital response. Academic Emergency Medicine. 1998 Jun;5(6):618–24.
Okumura T, Suzuki K, Fukuda A, Kohama A, Takasu N, Ishimatsu S, et al. The Tokyo Subway Sarin Attack: Disaster Management, Part 1: Community Emergency Response. Acad Emerg Med. Blackwell Publishing Ltd; 1998 Jun 1;5(6):613–7.
TPR: http://www.thepoisonreview.com/2017/02/24/did-the-nerve-agent-vx-kill-kim-jong-nam/
Part 2
this is James Warren Jones, best known as Jim Jones and the founder and leader of the Peoples Temple cult that came to fame in the 60s and 70s. Jones was a self confessed communism and started the church, not so much out of religious conviction but as a means to promote communism. This quote is useful “I decided, how can I demonstrate my Marxism? The thought was, infiltrate the church. So I consciously made a decision to look into that prospect.”

this was the Jonestown massacre of 1978. Jones had moved almost 900 of his church to Guyana to set up an agricultural settlement away from the threat of capitalism. On November 18th a delegation from the US congress visited Jonestown with concerns for human rights abuses. A small number of the congregation tried to defect back to the US. As the congressional delegation were on the airstrip to leave, Jones’ bodyguards opened fire on the delegation killing 5 people including congressman Leo Ryan. Knowing that this attack would bring the full wrath of the US upon Jonestown, Jones led a mass murder of his entire congregation of 900 people. This was something that they had actually rehearsed in advance on several occasions. There is a chilling audio track of Jones preaching to to his congregation persuading them of the need of this “revolutionary sacrifice”, with the murmurs of the kids and congregation in the back ground. Surrounded by armed guards people were encouraged to come and drink flavour aid mixed with valium, cyanide and chloral hydrate. Most took it willingly, giving it to their own children. 918 people died including almost 300 children.
cyanide acts as a mitochondrial poison. The mitochondria are the energy generating dynamos of the cell. The generation of ATP is dependant on the electron transport chain. Cyanide binds to the ferric (3+) ion of cytochrome oxidase a3. Shut down of this enzyme shuts down oxidative phosphorylation.
This is histotoxic hypoxia. With the electron transport chain cripple you can deliver all the oxygen you want and it just doesn’t get used. The cell switches to anaerobic metabolism and the usual toxicologic descent of coma, seizures and death.
we see this in two forms in the ED primarily. It is rare but if you’re going to see one in your career it’ll probably be inhalational via a house fire though there is a chance that you might see intentional ingestion as part of a suicide attempt in someone with access to chemicals (the jewellery manufacture injury is the most famous)
Diagnosis
the context is probably the number one clue as to what’s going on but there are a few others.
Cherry red skin, this is like whispering pectoriluquy or roth spots. historically interesting but rarely found. It does however illustrate a useful physiological principle. This is the visual representation of high venous oxygenation. Most of us have immediate access to VBGs – if the sats on your VBG are >90 then there’s a problem with oxygen uptake in the tissues
look for a high lactate. this is of course fairly non specific but once you start getting into lactates>10 in a house fire then cyanide has to be high up the differential
Management
Hydroxycobalamin is a precursor of vitamin B12. It has a cobalt moiety that has avid affinity for cyanide. This is best explained in the following complex chemical diagram
thiosulfate is commonly given as it’s fairly benign (though not effective enough to be used on its own in severe poisoning). it acts as a sulphur donor for the enzyme rhodanese which detoxifies cyanide into thiocyanate, once again easily peed out by the kidneys
dicobalt editate has been around for a long term and still has a place in the UK toxbase guidelines (it’s actually number one in severe poisoning). it chelates cyanide ions taking it out of play. unfortunately it can indue it’s own seizures and hyptensions, especially in those who have not actually been poisoned by cyanide
finally if you really want to screw with the physiology you can deliberately induce a methaemoglobinaemia using sodium nitrite. This produces a lot of Ferric Hb that acts as an attractive alternate binding site. Cyanomethaemoglobin is fairly safe compared to cyanide. However there’s a definite goldilocks phenomenon here where you want just enough MetHb to bind the cyanide but not too much otherwise you start getting all the side effects of MetHb which are of course seizures and hypotension. Never mind doing this in someone with coexisting COHb poisoning and all of a sudden you have a really interesting blood gas and an even sicker patient.
References:
Wikipedia on Jonestown: https://en.wikipedia.org/wiki/Jonestown#Deaths_in_Jonestown
Bebarta VS, Tanen DA, Lairet J, Dixon PS, Valtier S, Bush A. Hydroxocobalamin and sodium thiosulfate versus sodium nitrite and sodium thiosulfate in the treatment of acute cyanide toxicity in a swine (Sus scrofa) model. 2010 Apr 1;55(4):345–51.
Reade MC, Davies SR, Morley PT, Dennett J, Jacobs IC, Australian Resuscitation Council. Review article: management of cyanide poisoning. Emerg Med Australas. 2012 Jun;24(3):225–38.
Bebarta VS, Pitotti RL, Dixon PS, Valtier S, Esquivel L, Bush A, et al. Hydroxocobalamin and epinephrine both improve survival in a swine model of cyanide-induced cardiac arrest. 2012 Oct;60(4):415–22.
L P-CJ, J R, P VJ, S R V, P HC. Challenges in the diagnosis of acute cyanide poisoning. Clinical Toxicology. 8 ed. Informa UK Limited, trading as Taylor & Francis Group; 2018 Mar 15;0(0):1–9.
Part 3

this is edwin carter. On November 3rd 2006 was admitted to hospital with D&V and 22 days later died of multi organ failure ultimately related to Pollonium 210 poisoning

polonium 210 poisoning. edwin carter was the alias for former KGB agent Alexander Litvinekno. He released this photo shortly before he died saying, ”I want the world to see what they did to me”
Litvenenko was an officer of the KGB and latterly the FSB. He fled Russia following a book suggesting Putin’s rise was a coup organised by the FSB who he claimed had orchestrated things like the Moscow theatre hostage crisis
He was resident in London after claiming asylum and on the day he became ill he dined with two other Russians both former KGB in a sushi restaurant
On day 7 he disclosed his identity and expressed his concern that he might have been poisoned, on day 13 hr suggested radioactive thallium as a possible source (having seen that used during his time in the KGB). He had thallium testing done and a geiger counter was swept over his body which was negative. He developed progressive bone marrow failure.
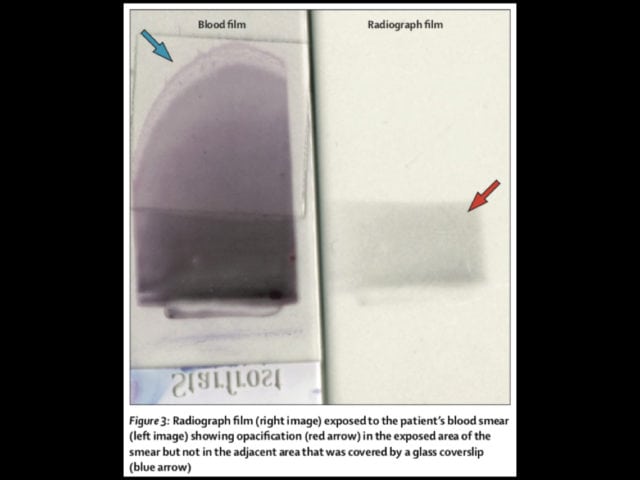
On day 22 a blood film was taken and part of it was covered with glass and part was left uncovered. this blood film was exposed to some radiographic film and the image on the right was produced suggesting that something in the blood was radioactive and it could easily be shielded by something as simple as glass. Later the same day he had gamma ray spectrometry that suggested polonium 210 as the likely agent. The same day he developed end stage multi organ failure and died.
This all comes from a great 2016 paper in the lancet published with the support of his family outlining the entire case. They estimate that in the 3 weeks from poisoning his liver alone was exposed to 140 grays of radiation, to put that in context a CTPA is around 0.015 grays
The most likely source was poisoning by one of the two former KGB agents that he met for lunch on the very first day. Likely this was something slipped into food or drink.
Polonium 210 is a radioactive isotope of the element polonium. It decays by the release of alpha particles to the stable Polonium 206 over several months. Was discovered by Marie Curie and named after her home country of Poland.
Types of ionising radiation

Dr Bruce Banner was exposed to large amounts of gamma radiation in an ill advised experiment and this produced the hulk. I saw it on TV so it must be true
Gamma radiation is like xray radiation and can penetrate all organs in the body but can be blocked by something like a big concrete wall. There are no particles involved this is a wave.

neutrons are sub atomic particles that are highly radioactive and released during things like nuclear detonations. they are highly ionising as one might imagine.

beta particles are a type of high speed election emitted by radioactive decay. They penetrate tissue but can be blocked by relatively simple things like wood. if anyone saw the TV series chernobyl – the extensive skin burns that many of the firefighters received were mainly from beta particles.
alpha particles consist of 2 protons and 2 neutrons bound together. produced as part of alpha decay of a radioactive substance. they can only pass a a few cm through the air and are easily blocked even by skin and are effectively non toxic unless inhaled or ingested. it is at least 20 times more ionising than gamma or beta. Plonium 210 is a potent releaser of alpha particles. once ingested this would not be detected by a geiger counter as the radiation was blocked by litvenenko’s own skin. the make shift blood film and X-ray film with the glass cover was a genius way of effectively showing that Litvenenko’s blood was full of alpha particles. there is a chelating agent for polonium 210 called unithiol but the lethal radiation dose in litvenenko’s case was probably reached hours following the exposure.
Like all of these cases, this is unlikely to be something you’ll ever see in your career. You definitely should not suspect polonium 210 poisoning in your next patient who presents with gastroenteritis. An unfortunately more realistic situation might be a terrorist related incident or a radiation exposure to someone in the industry. First thing is you will need help. This will be a big deal and radiation protection officers may well be informed before you are.
Depending on the context this may or not be needed. If your patient was exposed to something like pure gamma or X-ray radiation then there’s little role for decontamination as the radiation as passed through them and out the other side. They are no longer radioactive and the damage is done. If however there are concerns for beta or alpha particles involved (Chernobyl is a good example) then the patients are likely to be covered externally with radioactive dust containing these ongoing radioactive particles and they may well have inhaled or ingested more particles meaning that their blood and secretions likely contain ongoing radioactivity. A geiger counter can help in assessing external exposure to these things
Assessing the dose of radiation to the patient is important prognostically. There’s a couple of ways to do this but if you were to actually remember two things then:
- how quickly the lymphocyte count drops
- time to first emesis
a dose >5 gray puts you in the high risk for death.
References:
Wikipedia: https://en.wikipedia.org/wiki/Alexander_Litvinenko
1. Harrison J, Fell T, Leggett R, Lloyd D, Puncher M, Youngman M. The polonium-210 poisoning of Mr Alexander Litvinenko. J Radiol Prot. IOP Publishing; 2017 Feb 28;37(1):266–78.
2. Nathwani AC, Down JF, Goldstone J, Yassin J, Dargan PI, Virchis A, et al. Polonium-210 poisoning: a first-hand account. Lancet. 2016 Sep 10;388(10049):1075–80.