
These are some notes and references from a talk I gave at EuSEM 2019 in Prague. 
[Image from the Khajuraho monuments which have large segments dedicated to eroticism]
this talk deserves a little preface.
- when Christian first suggested the title to me it was “procedures gone wrong”, the fact that it happened to be in a session called “sex and the ED” didn’t quite click with me and i spent a little bit of time preparing a talk on CVCs gone wrong and misplaced tracheostomies. I thought i should really check to be sure and he confirmed that yes he did indeed want me to give a talk on sexual intercourse related injuries and misadventures. I cannot claim to be an expert in the issue though having produced 3 children I think i have managed to get the basic technique right.
- there is no way we can discuss this stuff without having a little giggle. From my point of view that is encouraged but i don’t think this the type of talk that might go down well online so I would perhaps caution the use of twitter throughout this talk as images and statements without context here might not be that helpful. There is a mixture of bad luck and poor decision making that leads someone to end up in the ED with presentations like these and no matter how much we might try to distance ourselves from such things we are all sexual beings and probably all of us have made decisions regarding sex that we regret at a later date.
Female genital Injuries
you’ll notice that this talk has covered almost exclusively male injuries. There are a few reasons for that. They’re common and dramatic and as a talk they can be quite entertaining. Female sexual injuries on the whole are a different story.
Many of them are relatively minor and women may well present to gynae as an OPD rather than the ED. If you see someone with vaginal or anal lacerations with a story of consensual intercourse then think twice. It may well be consensual but the literature is fairly clear that injuries to the female anogenital tract with intercourse are often non consensual and it’s worth delving a bit deeper into the history and using the same techniques you might for anyone with potential IPV. This may mean getting the partner out of the room it may mean raising it directly to the patient. Of course the same thing holds true for male injuries but the sad truth of it is that females are incredibly more likely to be raped and sexually trafficked than males are.
Lincoln et al suggests 10% injury rate with consensual and 55% injury rate with non consensual
Occasionally you will see a rupture of the vaginal wall that can cause significant external and internal blood loss and haemoperitoneum following intercourse is well described though often not that serious.
Congrats to the authors who managed to get papers with these titles onto pubmed.
Penile Fracture

i did a little bit of googling for this talk. Actually i’ll confess i did a lot of googling for this talk and honestly my browser history is not something i would like publicly shared at this point. But when you search penile fracture this is a common image that “pops up” no pun intended… It is of course something someone has put together on photoshop but it has been reused with great alacrity throughout a lot of the men’s sexual health type websites – usually with the label “penile fracture” and no sense of irony
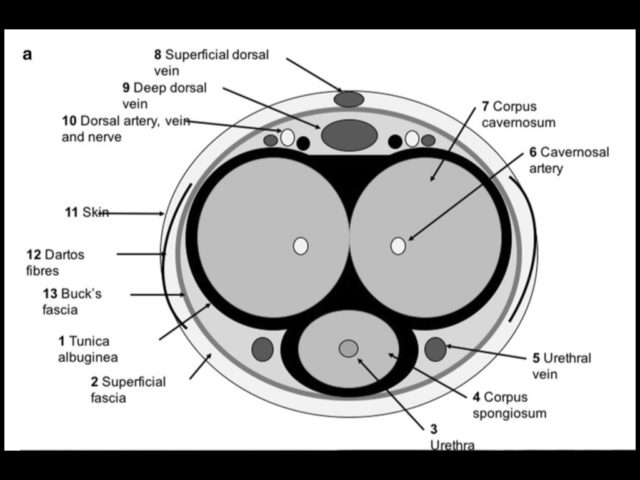
fracture is rupture of corpus cavernous and it’s tunica. usually proximal to mid penis on dorsal surface
we’re looking at three injuries in that context – 1) penile fracture, 2) urethral injury, 3) extratunical haematoma (which is a non surgical injury generally, and usually doesn’t have the crack and has a gradual rather than sudden detumesence)

risk factors for this include position with sources conflicting on this but with rear entry being higher risk than female partner on top being higher risk than male partner on top.
popping/cracking with rapid detumesence are the clinical features (along with pain). there is a small retrospective study looking at how important the sound is and they gave it an odds ratio of 4.25 and the absence of the sound decreased likelihood of surgical fracture from 90 to 70%.
imaging is not neccesarily needed but it can be useful to confirm diagnosis as there is a small number of pseudo fractures that probably do not need any surgery. timing of surgery is generally within 6-12 hrs. the integrity of the TA is the single most important predictor of need for surgical repair.
about 20% will have a urethral injury and blood and retention are the two give aways. these are difficult to diagnose and many end up with a retrograde urethrogram or a cystoscopy
ED Management
- analgesia, penile blocks might be useful but i would get urology involved first
- do not catheterise if they’re in retention – it’s a sign of urethral injury and just like pelvic fractures you’re likely to make it worse
- get urology involved. They may well want an ultrasound and that’s reasonable but probably not someone to send home to come back to clinic in a few days.
Vacuum Related Injuries
these are worth discussing as they do seem to be reasonably common and come with a reasonable degree fo morbidity.
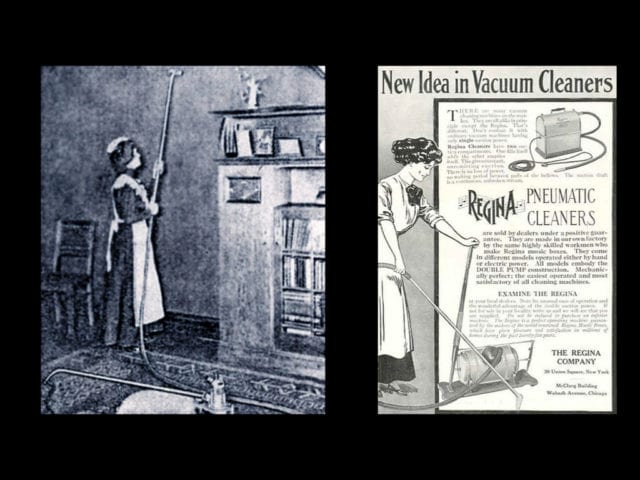
vacuum cleaners have been around since later 19th century when they were bellows operated and obviously fairly poorly understood as this poor maid on the left is demonstrating while trying to hoover the wall…
by the 1950s these were fairly common appliances to have around the house.
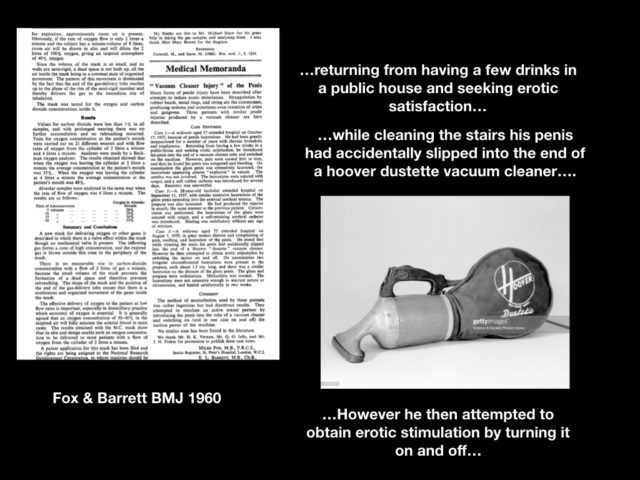
I can see why he might claim accident but if you’re gonna claim your penis got stuck in there by accident then you may as well commit to the story…
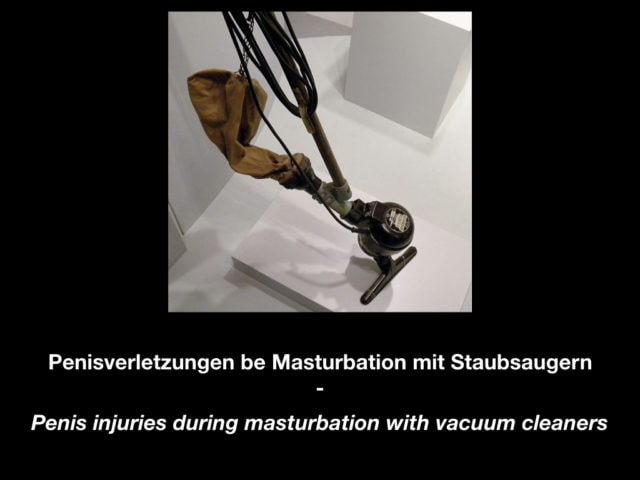
in 1978 a munich based urologist wrote a dissertation called … reporting a series of 16 men who had been injured while pursuing erotic stimulation with the Vorwork made Kobold vacuum cleaner. this translates as
Penis injuries during masturbation with vacuum cleaners
The rotating turbine of the cleaner was positioned close enough to the inlet of the pipe that as the penis was drawn into the vacuum the glans would become lacerated by the rotating turbine.
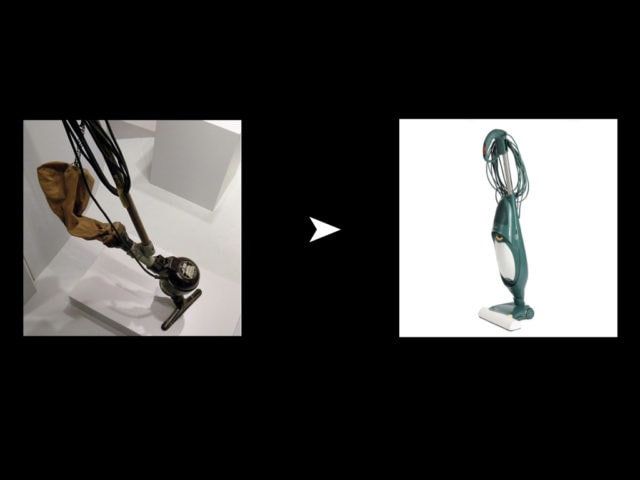
normally in the world of obscure academia that would be that but given the title and the fact that we like laughing at penis related injuries – the dissertation took on a life of its own becoming widely known in Germany ultimately “climaxing” in a spoken word tour of germany where two actors literally did a reading of the dissertation. It is now available as an audiobook. In terms of knowledge translation you’ve got to admit that’s pretty good through it still did take 33 years before the audiobook was finally publihsed. to give credit to vorwork – as soon as the dissertation was published they updated the model of the cleaner meaning that the particular described injuries would no longer be possible
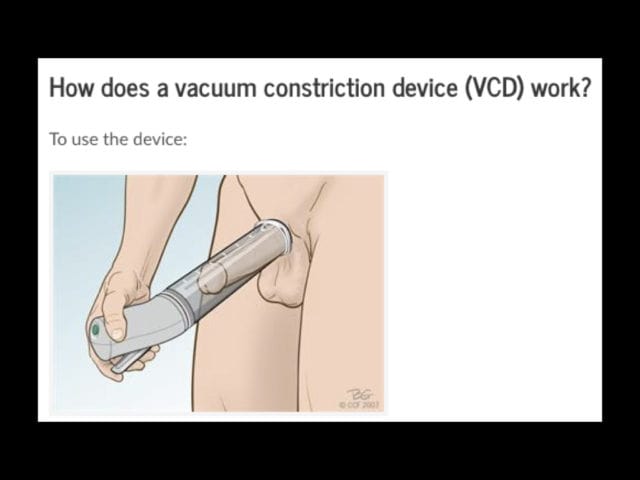
it must be said that these poor patients that were being parodied across the pages of the BMJ were actually somewhat ahead of their time. ultimately today vacuum constriction devices are recommended as one of the myriad treatments of erectile dysfunction. so if a patient says that their doctor told them to put their penis in a vacuum cleaner then there is a little nugget of truth in there somewhere
Priapism
can be sexual related or…
- can be medical or sickle/leukaemia
- drugs associated are
- antipsychotics (apparently have alpha blocking effects)
- antidepressants
- alpha blockers
- time dependant factor needing intervention
- two forms, low flow (common) and high flow (spinal)
lots of the sexual related priapism are from injectable agents. This is a well established therapy and is self administerd into one of corpa and diffuses to the other. Usually alprostadil (PGE1) or papaverine (phosphodiesterase inhibitor). 5-10% get priapism
Iin the case of priapism from injectable substances injecting something like phenylephrine (0.1-0.5 mg/ml concentration in 1 ml boluses up to total 1mg) can help (UroWeb has this as first line). Follow this with aspiration from each corpus. 50mls is a reasonable number. Remember there are 2 corpus cavernosa, one on each side so they need separate aspirations
Genitourinary Foreign Bodies
this is an ED favourite and i’m sure all of us have various stories that we’ve been involved with. there’s obviously a lot of stuff that can be inserted into a rectum but i just don’t have time to cover any additional orifices for now.
Van Ophoven et al is a great reference for this.
They begin with a short review of things applied externally to the penis and are willing to horrify readers with the above image of a large hex nut applied to the base of the penis.
they even describe (a now thankfully outdated practice) whereas newlywed brides would place a wedding ring over the penis following wedding night coitus as a means of ensuing potency for life. and i know size isn’t everything but one imagines if a wedding ring fits over it that easily that potency would perhaps be the least of your problems.
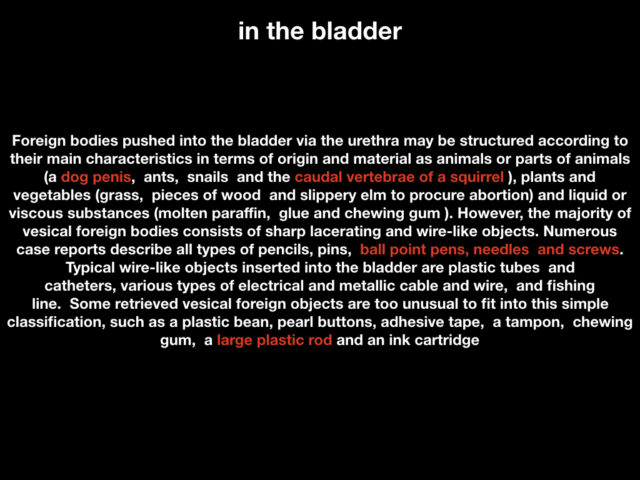
they then move onto a staggering list of objects documented in the literature that have been found first in the urethra…
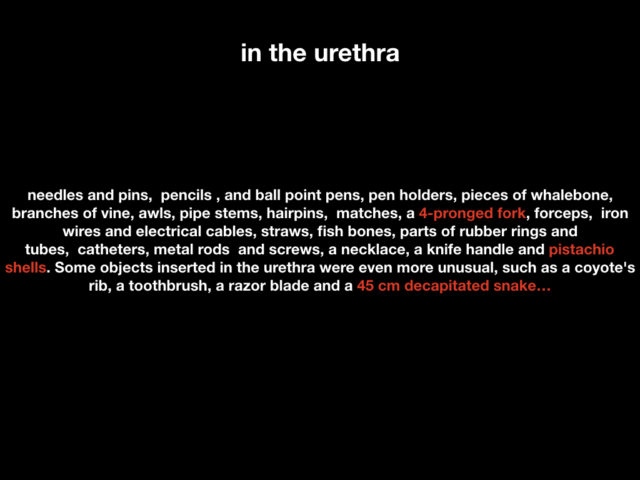

when presented with this the obvious thing would be just to pull the damn thing out, however it is sods law that whatever got shoved in there has immediately tied itself in a knot and refuses to come out. in this case report i am assured that the keys are in his pocket and they just didn’t pull his jeans down. Which i must say given the nature of the X-ray request does seem like the pinnacle of doing your job badly
ED management to be honest is fairly simple and the key thing is don’t make it worse being too aggressive in removal. Get urology involved, get some imaging. Depending on what’s there they meed a urthethotomy to remove a distinct small FB from the urethra or in the case of the tangled cable they often need advanced so the entire object is in the bladder and then removed via an incision through the bladder itself.
Anaphylaxis to Semen
The case:
A 32-year-old woman was admitted to our emergency department because of an abrupt onset of hives characterized by periorbital redness and swelling, breathlessness, and wheezing. Angioedema and hypotension (90/60 mmHg) were observed.
yes believe it or not this is actually a thing. this is very niche and rare (about 80 cases in the literature) and unlikely to be something you’ll ever see. but it is kind of fascinating. It appears to be typical IgE anaphylaxis to some glycoprotein content of the seminal fluid plasma – not the sperm itself. So ideally you can still get pregnant through artificial insemination if you spin off the plasma. I had a reasonable look at this but I couldn’t find a clear answer to the question – is it all semen or just your current partners. cause if it’s just your current partner’s then maybe it’s time to consider a change.
This case report is one among many and i hesitate to call it the “seminal” paper on the topic…
Not only did they diagnose it but because the women wanted to conceive naturally with her husband rather than artificial insemination. So they did what all could allergists did and did local desensitation by injecting subcutaneous plasma of the husbands seminal fluid until there was no reaction. They sent them home with a bottle of wine and an epipen and told them to make babies. Which they subsequently did.
It also seems possible to be anaphylactic to penicillin even if you yourself have not been taking the penicillin but are indeed exposed to it via your partners semen. you know the way the antimicrobial stewardship people in your hospital always want lots of details about the penicillin allergy – well i’m not sure they want this much detail.
Neurological Events
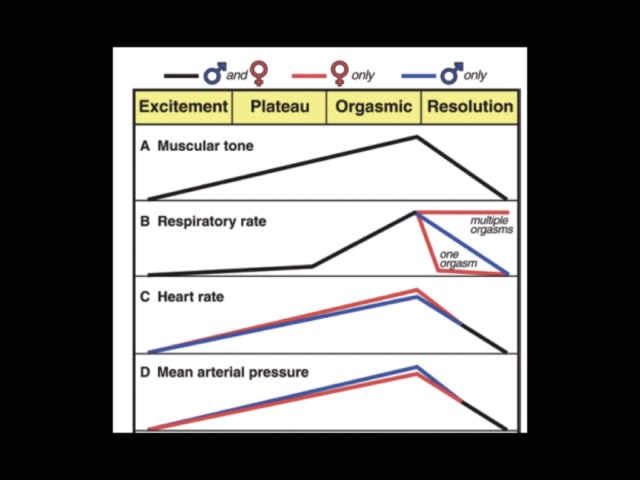
The link between sexual climax and SAH is well described. The image above is from a paper looking at aneurysm rupture and sex. it seems to be linked to spikes in BP at orgasm (up to 100 spike in the systolic in men). this is all based on data from the 50s from these two:
Much of what we know about human sex physiology and orgasm comes from this husband and wife team in the 50s. Virgina Johnson and William Masters. I kid you not – the world’s leading sex researchers are called Virginia Johnson and Willie Masters. You cannot make this stuff up…
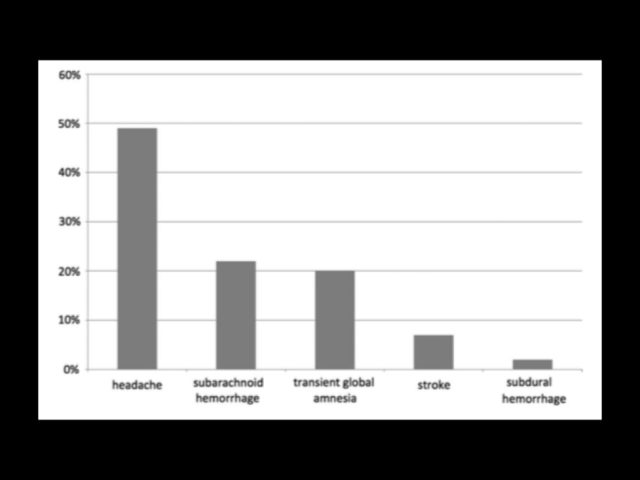
In one series of neuro diagnoses presenting to the ED the diagnosis was most commonly coital headachefollowed by SAH, followed by TGA. They all need investigated, don’t worry but it’s OK to advise patients that while this sounds like a worrying headache it’s probably not.
I have to say that TGA following intercourse is probably an evolutionary adaptation of post coital regret depending on your reflections upon your choice of the previous evening’s sexual partner
References:
Lincoln C, Perera R, Jacobs I, Ward A. Macroscopically detected female genital
injury after consensual and non-consensual vaginal penetration: a prospective
comparison study. J Forensic Leg Med. 2013 Oct;20(7):884-901. doi:
10.1016/j.jflm.2013.06.025. Epub 2013 Aug 15. PubMed PMID: 24112341.
Reynolds MR, Willie JT, Zipfel GJ, Dacey RG. Sexual intercourse and cerebral aneurysmal rupture: potential mechanisms and precipitants. J Neurosurg. American Association of Neurological Surgeons; 2011 Apr;114(4):969–77.
Lee J, Kim S, Kim M, Chung Y-B, Huh J-S, Park CM, et al. Anaphylaxis to husband’s seminal plasma and treatment by local desensitization. Clin Mol Allergy. 2008 Dec 5;6(1):1081–3.
Deria M, Rizk C, Desormeaux J, Santucci S, Karsh J, Bernstein J, et al. Seminal fluid anaphylaxis. Allergy, Asthma & Clinical Immunology. 2011 Nov 14;7(S2):A39–1.
Pfortmueller CA, Koetter JN, Zimmermann H, Exadaktylos AK. Sexual activity-related emergency department admissions: eleven years of experience at a Swiss university hospital. Emerg Med J. 2013 Sep 7;30(10):846–50.
Bunzel L, MD SCK, MD BZ, PhD MAV, MD MP. Non-Natural Death Associated with Sexual Activity: Results of a 25-Year Medicolegal Postmortem Study. The Journal of Sexual Medicine. Elsevier Inc; 2019 Aug 20;16(10):1–10.
Cavalcanti AG, Krambeck R, Araújo A, Rabelo PH, Carvalho JP, Favorito LA. Management of urethral lesions in penile blunt trauma. Int J Urol. 2006 Sep;13(9):1218–20.
Gaspar SS, Dias JS, Martins F, Lopes TM. Sexual Urological Emergencies. Sexual Medicine Reviews. 2015 Apr;3(2):93–100.
Benson RC. Vacuum cleaner injury to penis: a common urologic problem? Urology. 1985 Jan;25(1):41–4.
Lewi H, Drury JK, Monsour M. Vacuum cleaner injury to penis. Urology. 1985 Sep;26(3):321.
FOX M, BARRETT EL. “Vacuum cleaner injury” of the penis. Br Med J. British Medical Journal Publishing Group; 1960 Jun 25;1(5190):1942–2.
Ory J, Bailly G. Management of penile fracture. CUAJ. 2019 Jun 10;13(6S4):1–3.
Cozzi D, Verrone GB, Agostini S, Bartolini M, D’Amico G, Pradella S, et al. Acute penile trauma: imaging features in the emergency setting. Radiol med. 18 ed. Springer Milan; 2019 Jul 12;19(6):1–11.
Dias-Filho AC, Fregonesi A, Martinez CAT, Pimentel ES, Riccetto CLZ. Can the snapping sound discriminate true from false penile fractures? Bayesian analysis of a case series of consecutively treated penile fracture patients. IJIR: Your Sexual Medicine Journal. Springer US; 2019 Sep 21;6(4):1–9.