
A chap with a 6 month old ileal conduit for urinary diversion rocks up to your ED feeling more than a little unwell.
A VBG done at triage is like this:
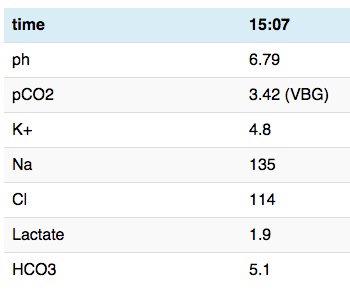
What’s the deal?
The reference
Tanrikut C, McDougal WS. Acid-base and electrolyte disorders after urinary diversion. World J Urol. 2004 Jul 29;22(3):168–71. [PubMed]
[peekaboo_link name=”Types of urinary diversion”]Types of urinary diversion[/peekaboo_link]
[peekaboo_content name=”Types of urinary diversion”]
- you can make a urinary diversion out of lots of bits and bobs lying around in the abdomen. I’m sure there’s a very technical side to choosing which bit or bob to use
- gastric
- jejunum
- ileum and colon (this seems to be what I see)
[/peekaboo_content]
[peekaboo_link name=”General issues”]General issues[/peekaboo_link]
[peekaboo_content name=”General issues”]
- decline in renal function (thought to be due to obstruction and reflux)
- infection
- stones somewhere along the system (which are linked to infection)
- metabolic disturbances – this is the interesting one we’ll tackle today
[/peekaboo_content]
[peekaboo_link name=”Metabolic disturbances”]Metabolic disturbances[/peekaboo_link]
[peekaboo_content name=”Metabolic disturbances”]
- normal bladder does not alter the urine – there are no funny ion pumps changing concentrations and fiddling with your wee wee
- whichever section of gut your urologist
randomly plucks from within the abdominal cavitychooses their venous drainage will all be to the liver. This can be an issue if your urinary diversion starts sending lots of urea to your liver especially if it’s already struggling. - this all changes when you use a bit of gut and different bits of gut cause different issues
- if you use stomach then you can get a hypochloremic metabolic alkalosis
- imagine it a bit like continual vomiting with Cl loss
- you can even use PPIs to reduce the action of the H+/K+ pump and reduce H+ loss thus lowering the pH again
- if ileum or colon then you get a hyperchloremic metabolic acidosis. There is net absorption of both ammonium and Cl back into the circulation that was just trying to get rid of it.)
- if you use stomach then you can get a hypochloremic metabolic alkalosis
- Minimising contact time reduces all of these. If the urine isn’t in the pouch for very long then the acid base problems don’t happen. If this is happening then you have to question how well the urinary diversion is working.
[/peekaboo_content]
[peekaboo_link name=”Management”]Management[/peekaboo_link]
[peekaboo_content name=”Management”]
- probably one of the few occasions where bicarb is the right answer
- though rapid correction of pH with bicarb will drastically alter your potassium in these patients and thus create a “clean kill” as we say. Just like DKA you need to watch the potassium and in general here we mean potassium replacement as the pH comes up
- in terms of ammonia and possible encephalopathy the treatment is drainage – get the urine flowing and the liver should catch up.
[/peekaboo_content]