
This is based on Mark Wilson’s paper in the Journal of Cerebral Blood Flow & Metabolism [Free full text] which i’m sure you all read avidly every month.
COI – I know Mark and had the honour being in the same speaking track as him when he gave a similar talk at SMACC Gold. He was very kind and didn’t point all the things I was wrong about in my talk.
I learned lots from this paper and it turns out there are lots of subtleties to ICP that the classic Monroe-Kellie doctrine doesn’t account for. Level of evidence is as you might expect somewhat low but this is fascinating stuff none the less.
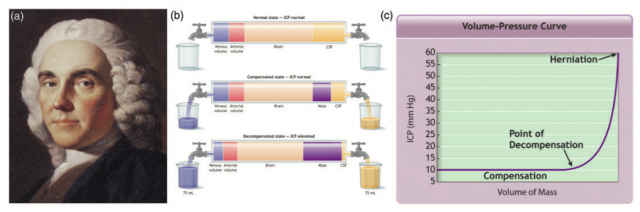
What is Monro-Kellie?
- Monro (Scotsman with dodgy wig) suggested that skull was a closed box and as soon as you add something to the box either pressure goes up or something gets squeezed out
- Kelli (Monro’s student) did some autopsy work suggesting Monro was right.
[collapse]
Problems with Monro-Kellie (apart from the dodgy wig...)?
- blood and CSF given the same weight/importance despite the fact that CSF production and flow is tiny and venous flow is huge (equal to arterial inflow at 14% of the cardiac output)
- it therefore makes sense that a problem with venous outflow or accumulation is likely much more important than CSF.
- there has been lots of focus on managing the arterial side of things with certain CPP goals that entirely ignore the fact that fiddling with the arterial side when there’s a problem with outflow might miss the point.
[collapse]
Tell me about these veins then
- i did a podcast on it once…
- most people have asymmetric venous drainage and are quite dependent on their dominant side – if this side gets obstructed (maybe by a depressed skull fracture) then that’s probably important
- they’re formed by little dural folds with no support of their own (unlike the muscular arterial walls) and are hence very dependent on their surroundings. Eg, next time you’re opening a dural sinus in someone sitting upright it’s worth remembering that the dural sinus pressure is probably negative and will cause a massive air embolism. Likewise when you lie someone flat the venous sinus engorges.
[collapse]
What causes problems with venous drainage or venous hypertension?
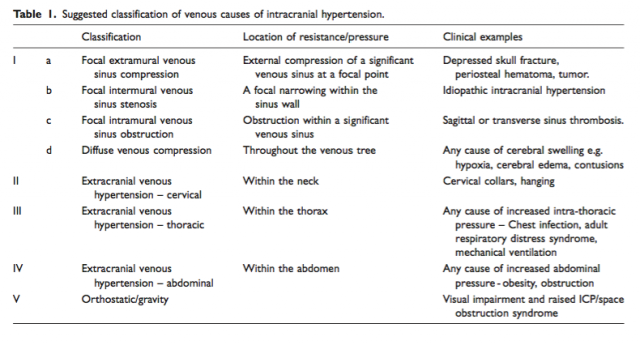
Mark provides a lovely little classification in the table above
[collapse]
Some pearls
- a depressed skull fracture over a venous sinus (esp a dominant one) may cause venous outflow problems worsening ICP. The venous sinus may even thrombose
- idiopathic intracranial hypertension (that disease of young obese women with papilloedema) is associated with venous sinus stenosis
- poor head position (slight flexion and rotation) will significantly impair jugular (and hence intracranial) venous drainage. Not to mention the dreaded collars…
- outside the head, high ventilation pressures transmit to the venous system and indeed even raised abdominal pressure can cause refractory raised ICP (as beautifully described by Tom Scalea
- even microgravity causes issues with astronauts reporting a syndrome somewhat similar to idiopathic intracranial hypertension during prolonged time in space
[collapse]