
Podcast: Play in new window | Download (Duration: 7:42 — 10.9MB)
Subscribe: Apple Podcasts | Spotify | RSS
Welcome back to the tasty morsels of critical care podcast.
This time we’re looking at pulmonary hypertension. Mainly cause I recently had to give a talk on it so it’s fresh in my rapidly diminishing brain cells and thought I should get it all written down before I forget it. We’re going to try it as a 2 parter. Part 1 will cover a broad overview of pulmonary hypertension and part 2 will focus on management strategies for a PH patient in the ICU.
Saying a patient has PH does not really tell you very much. All we mean is that pressures in pulmonary circulation are higher than they should be. Saying someone has PH and not quantifying it is a little like saying someone has cancer but not saying which organ or how advanced it is. We need to go a bit further than just say they have PH and quantify the cause or rather which group of PH they’re in. We also need some way of quantifying the severity of it.
The definition of PH since the 2022 ESC guidelines is a mean PAP of 20mmHg on a right heart catheter. Echo can be used to screen for “probability” of PH but the right heart cath is needed to make the diagnosis. Once you’ve defined that the pressure is high the real doctory work begins as you have to figure out the likely cause. The language the guidelines use is “group”. You should be able to put your patient into 1 of 5 groups.
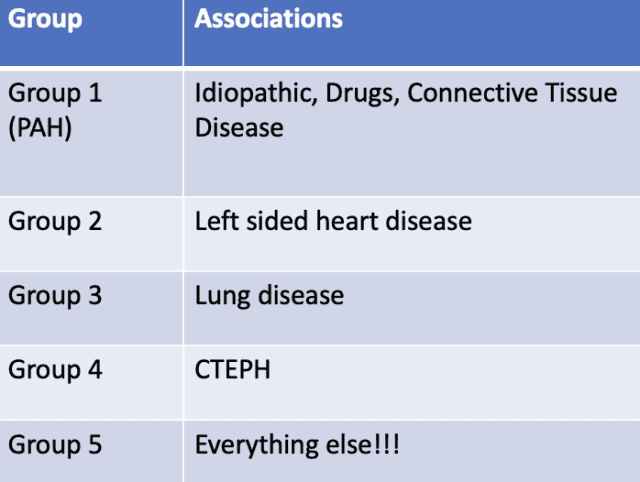
To give an example you are handed over someone who has known PH. You dig a little deeper and see they have an mPAP of 27 on a recent right heart cath. Their echo shows a poorly functioning LV and severe MR. The PH here is going to be group 2, PH secondary to left heart disease. This is by far the commonest.
Or another example, you are told someone has PH. You dig a little deeper and see an echo report that says the left heart works well but the right side is dilated. You dig a little deeper and see the clinic letters describing severe end stage emphysema. This is likely to be group 3 PH, PH secondary to lung disease.
In both those examples the PH is a problem but it is a downstream effect of other disease. And unless you can fix the heart or lung disease then the patient is in trouble, indeed if the patient dies in the coming weeks to months it’s likely going to be the left heart disease or the lung disease that kills them.
Let’s spend a few minutes talking about group 1 PH, sometimes called PAH. This is rare but often very severe and progressive and comes with some unique medications so it’s worth discussing. These people should have normal lung parenchyma and normal left hearts. There are a variety of specific causes in group 1 but a lot of it is described as “idiopathic”. It is a progressive pulmonary vasculopathy where the tiny arterioles suffer intimal proliferation and eventual fibrosis due to a variety of vasoactive molecules. This transforms the pulmonary circulation from a very compliant, low resistant circuit into a narrow and stiff group of pipes. The right heart is evolved and very comfortable with assisting large volumes of blood through a low resistance circuit. In hroup 1 PH, the change in pulmonary vascular resistance is more than the right heart can cope with and the right heart over time starts to fail in its primary purpose of maintaining a low CVP while delivering preload to the LV.
Over the past decades a number of classes of drugs have been developed that target the vasoactive molecules that cause the vascular changes. These can be split into 3 classes
1) endothelin receptor angtagonists which do exactly what the name says: reducing endothelin. Drugs like macitentan fall in that category
2) PDE5 inhibitors. These inhibit the enzyme you expect from the name but the key outcome is that there is an increase in nitric oxide something that causes pulmonary vasodialtion. Sildenafil or tadalafil are two common drugs in this group
3) prostacyclins. These vasodilate and reduce proliferation in the vascular bed and typically IV epoprostenol is the drug of choice here.
These drugs have proven disease modifying benefit but only in group 1 PH. We have not been able to prove any benefit for those with PH from left heart disease or lung disease. The more severe their disease the more drugs they might be on. Some patients are even on IV epoprostenol in the community to keep their PVR compatible with life.
These 3 classes of drugs have had a significant impact on both length and quality of life in PH. But the prognosis in group 1 PH is still one of progressive irreversible disease in the longer run. There are lots of features that are well validated on an outpatient basis to determine prognosis however that is rarely the question we’re faced with. For example we know ICU admission is a poor prognostic sign in severe PH but this is generally the very point we get involved at. As usual i suspect decisions about prognosis in the ICU setting are typically decisions about limitation or withdrawal of life sustaining therapy and they all depend on reversibility. If someone with severe PH has a pneunonia then we can probably turn that around then that’s something to consider. However if the right heart and liver are failing due to worsening congestion from progressive PH then that’s a different question.
That’s enough for today and to give you an overview of PH, next time we’ll focus on some management strategies.
Reading
My own rambling review of pulmonary hypertension on JFICMI website.