
My experience with US is mainly self-taught when I spent long ICU shifts performing echos on every patient in the unit. I’ve done my level 1 course but the accreditation process ain’t that easy in Ireland, and particularly where I worked it’s all very new. Trail blazing is hard work.
Anyhow.
Previously looking for an FB was either some LA and hoking around with a blade and forceps or we got radiology to scan them (a challenge in itself) and they’d leave us a nice x marks the spot and then we’d start digging on it.
This is hardly ideal.
I’ve read some stuff on locating FBs with US and figured I’d just have a go (this is common though perhaps worrying trend in my practice…)
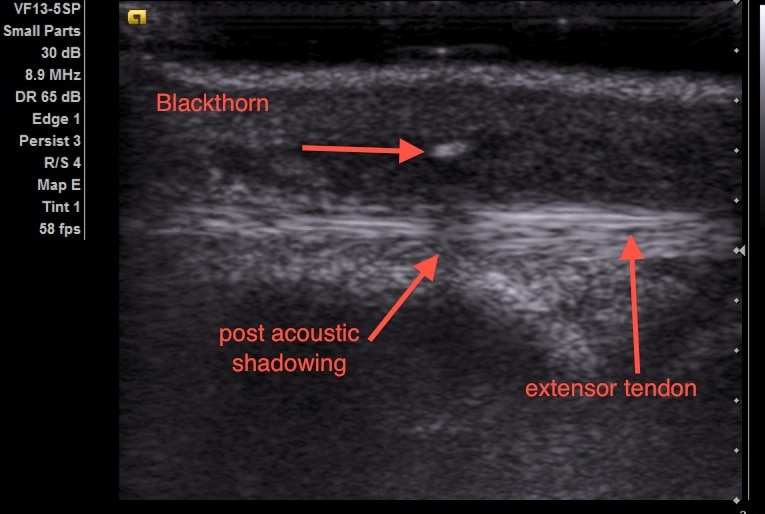
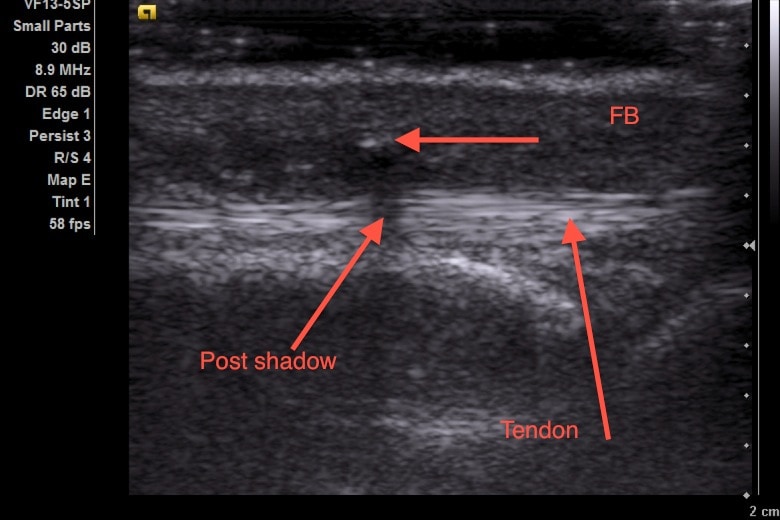
I got images like these.
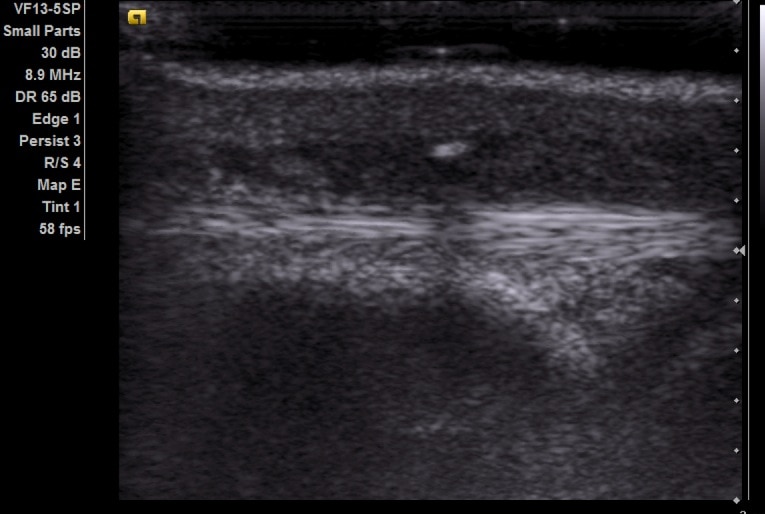
You can place a needle under visualisation in long axis until the tip is on the FB.
You can then just make an incision along the shaft of the needle till you find the FB


I’m pretty sure I’d picked up the idea of using the needle to cut down onto from somewhere but I’ve no idea where. Anyone know anything published or on the web about that?
There’s a fair amount already published on the use of usltrasound FBs but I’m not aware of any randomised trial out there. Not that I’m really sure we need one but it’d be nice to know.
Ultrasound Village have a similar case (with a much more substantial FB!)
And this paper is worth a read too if you can get it.
UPDATE: @e_med_doc suggested this great paper. It has lots of nice images of using the needle to get down on the FB.
Welcome to the EM blogosphere, great posts!
Really like your approach of self-learn and go… I am in the same situation. The clinic has paid me a FAST course but I will never in my life have all the courses to learn all the applications of ultrasound that I want to learn. By learning from online texts and videos and doing some self-experimenting I’m getting on the learning curve. It’s just like the stethoscope – examine hundreds of patients until you know the difference from pathological and normal. I am careful not to use the ultrasound for definitive diagnosis or rule-out but a rule-in so that I can make a better plan on how to approach the patients symptoms. I cannot see any difference in doing this with the sonar or the old stethoscope where all doctors are falsely assumed to be skilled masters hearing every heart sound and murmur there is. At least, the online educational material for US is much better and easier to replicate by storing the images!
Regards,
David
ps my blog is a bit empty after having my third child this winter, I’m slowly getting back to normal life – and blogging
Hi David
thanks for the welcome, I’d had a look at your site in the past and noted the lack of activity but the third child certainly explains things!
there is some cracking stuff on the net on US isn’t there
rule-out stuff is a bit tricky with the US so i agree that certainly for now I’ll only be using it in the rule-in or procedural way
andy
Really like the pics. Any idea what the FB was or how it got there?
Hi
Thanks for the comment.
The fb was a thorn off a branch when he was gardening. About 2mm long.
Funnily enough I had a fairly similar case today. I’ll try and post the scan from it. I’ve taken to dunking hands in basins of water and scanning them in the water and it gives a far nicer picture.
Pingback: The LITFL Review 021 - Life in the FastLane Medical Blog
Hi,
Totally agree with your situation here. I am working in a small missionary hospital in North India and was faced with same situation here where a female 50 yrs, presented with a non healing chronic sinus which formed after she took a fall in her house before 2 months. She went to several hospitals prior to coming here and was just on regular daily dressings. For first instance even i thought it was perhaps just a case of chronic osteomyelitis, however nothing much on the xray. Out of curiosity, i performed the superficial USG of the forearm and to my surprise unsual solid focal leison with strong acoustic shadowing was seen between both the bones. Prompt probing under LA and after an hour ordeal, a wooden sharp FB was taken out 9-10cm in length. So i would say USG is the handy instrument of the day!
Dr Paul Anant
Hi Paul, that’s a great case – 10 cm is a pretty huge FB! I can imagine she was grateful for the removal.
Yeah was an interesting case. USG with linear probe on superficial mode is quite helpful for me in FB detection. I have qualified as General surgeon however i am very interested in EM, so perhaps will take it as my second training if i get a formal training place.
Pingback: More thorns in the flesh - Emergency Medicine Ireland
Pingback: The LITFL Review 021 - LITFL