
From one of our national training days with an excellent MSK radiologist
Some of this is more UK/Irish specific as access to sports medicine and MRI imaging for MSK conditions is really difficult and a lot of patients are forced into the private system. This is somewhat above and beyond standard EM but as Swadron says we need to know what we need to know and one step beyond.
This information will hopefully help you investigate and manage the poor souls who in desperation end up in our EDs
A case
A 20 year old male playing county level sport (take your pick) presents complaining of increasing right hip pain during and after sport. He has attended his GP, had an xray, had a course of physio and is taking an NSAID all with little relief and is now unable to train or play.
What is the likely pathology here?
Femoral Acetabular Impingement
- the young patient with grumbling hip or commonly groin pain. Usually with flexion/adduction
- we (and I!) used to call this type of thing Gilmore’s groin – there’s some debate whether this is accurate and it may well be a hip problem.
- femoral acetabular impingement is an umbrella term
- 20% of people have some degree of femoral head abnormality (The Pun et al paper below gives roughly this figure in asymptomatic adults)
- these abnormalities fall into two categories
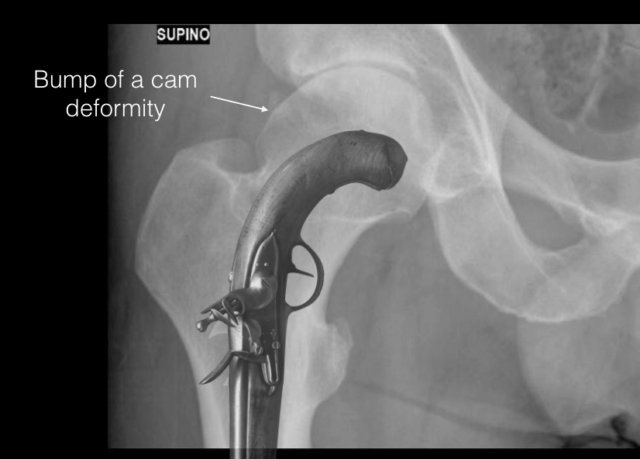
- 1) a CAM deformity
- the head and in particular the neck is too big for the acetabulum resulting in contact at the anterosuperior labrum with flexion and adduction
- also known as a pistol grip deformity
- ultimately these can result in a substantial labral tear which is often something needing surgery and can end up with accelerated OA and an early hip replacement
- 1) a CAM deformity
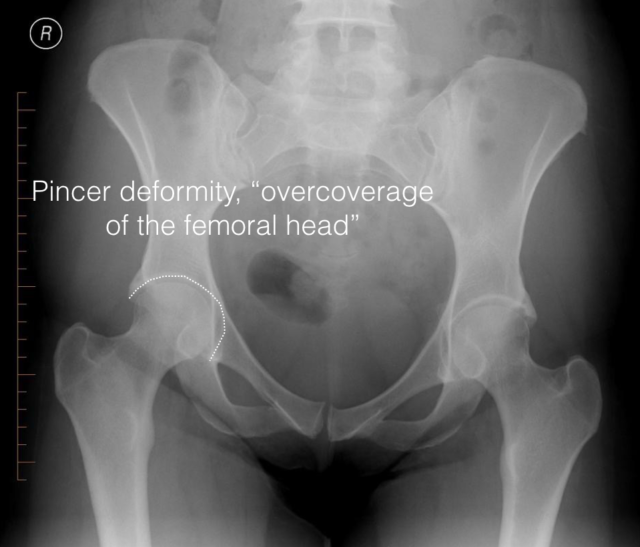
- 2) a pincer deformity
- this is more where the acetabulum is too big for the head
- the neck as it swings up now hits the acetabular edge and over time causes a stress fracture at the superior edge of the acetabulum. The old roentological variant book (Keats) would often label things like these as normal variants. In the age of the MRI we now know they’re fractures.
These abnormalities and subtle and often won’t be commented on by radiology unless they’re really looking for them (remember to always give full clinical details and a specific clinical question). Even then xray is not a great test for this and just because the xray is reported normal doesn’t mean you shouldn’t seek further imaging.
You may have been expecting and wanting some info on what to actually do with this lovely new information but the talk was on radiology and diagnosis, not management. Sorry…
Further Reading:
- Radiopaedia (as always) have a nice article on this
- Pun S, Kumar D, Lane NE. Review: Femoroacetabular Impingement. Arthritis & Rheumatology. 2014 Dec 27;67(1):17–27. [Full Text PDF]
- Agten CA, Sutter R, Buck FM, Pfirrmann CWA. Hip Imaging in Athletes: Sports Imaging Series. Radiology. 2016 Aug;280(2):351–69. [Abstract]
If you have access then there’s a nice up to date article.
Pingback: Tasty Morsels of EM 068 – Femoral Acetabular Impingement – Global Intensive Care