This is uncommon, not something you’re going to be diagnosing or even suspecting on a day to basis.
Two main causes
- malignancy 80%
- thrombosis 20%
For malignancy think right sided lung and mediastinal masses. Anything that can compress the SVC as it returns to the right atrium
Classically this will be non small cell lung cancer followed by non Hodgkin lymphomas
For thrombotic causes then there’s usually a precipitant in the form of an indwelling line
- dialysis, port, Hickman, pacer etc…
- this is the same as for upper limb DVT in general – there’s usually a cause.
A big clot in the major veins returning to the heart would be expected to be a big cause of PE but this seems uncommon. There also seems to be a differentiation between clots on the line (sleeve thrombi) which more commonly cause PE, as opposed to clot on the wall (mural thrombus) which embolisms much more rarely.
Presentation
- dyspnoea the commonest (presumably a mixture of reduced venous return and neck vein distension)
- usually there are facial changes – swelling, redness, especially with bending forwards
Investigations
- CXR usually abnormal (though up to date quoted 85% only)
- ultrasound can usually only view the vessels immediately proximal to the SVC but you can get indirect information by looking at Doppler waveforms with a valsalva (you were all doing that already for your DVT scans weren’t you…)
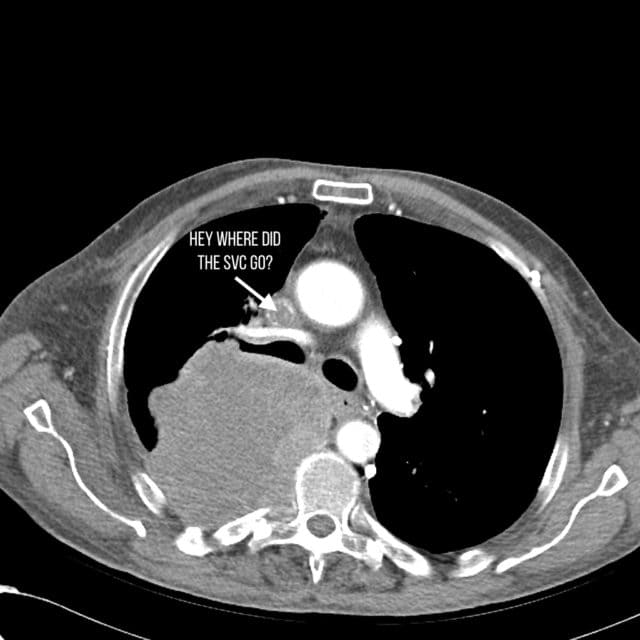
- unsurprisingly CT is the best test as the key treatment decision is finding out whether this is a malignant SVC obstruction vs a thrombotic SVC syndrome
- the next major treatment decision point is biopsy if malignant. The decisions regarding radio and chemo that the oncologist will be driven by this.
I mention the last point to emphasise that while this is an important cancer emergency the time scale is quite different from something like neutropenia sepsis.
In health systems where access to CT at 2am is limited then this is a CT that can wait. SVC is rarely an immediately life threatening emergency and intervention (such as stenting, radio, biopsy and chemo) can all wait till daylight and as a result the CT can probably wait till morning too.