
I’m entering a few months prep for the UK and Ireland exit exam in Emergency Medicine: the FRCEM. I’ll be adding lots of little notes on pearls I’ve learned along the way. A lot of my revision is based around the Handbook of EM as a curriculum guide and review of contemporary, mainly UK guidelines. I also focus on the areas that I’m a bit sketchy on. With that in mind I hope they’re useful.
You can find more things on the FRCEM on this site here.
These are rare but still important and of course very testable. Questions might concern fever in a returning traveller or specific questions about specific conditions. I’ve covered malaria already and I’ll cover MERS-CoV and ebola in a later post
(From the OHEM)
- <1 week
- Cholera: 1-3 days
- Dengue: 4-7 days
- Yellow fever: 3-6 days
- Most of the diarrhoeal ones are less than 1 week too
- 1-3 weeks
- lassa fever: 1-3 weeks
- leptospirosis: 1-2 weeks
- malaria: 1-2 weeks (can be longer of course)
- typhoid: 1-2 weeks
- >3 weeks
- most of the hepatitides (?)
- amoebiasis: weeks to months
- rabies: usually 3-12 weeks
(from Public Health England)
- a viral encephalitis
- often bites
- can be inhaled in caves with bats
- in the UK
- Clinical features
- pain and tingling at wound site (remember this will be over 3 weeks down the line)
- headache fever
- spreading paralysis
- hydrophobia – muscle spasms with drinking water
- almost invariably fatal once symptomatic
- Management of a potential exposure (in this case a bat)
- barrier nursing
- vaccination status
- nil
- partial
- full (noted as at least 3 of 5 doses)
- type of exposure
- no physical contact
- uncertain contact (eg a child in a room with a bat)
- direct contact with saliva (eg a bite)
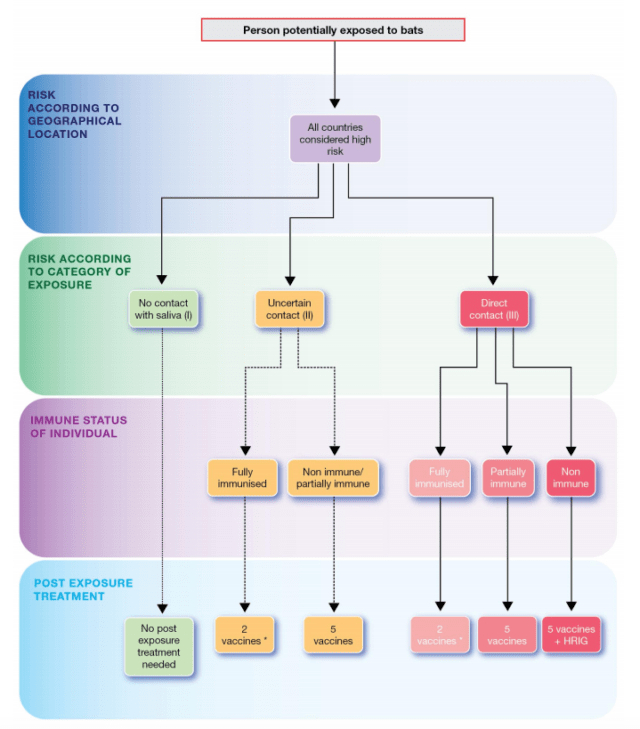
- for us the likely case will be an uncertain contact with no prior vaccine. In which case the answer is 5 vaccines.
- The only time we’re going immunoglobulin is definite contact and no vaccine.
- How are the vaccines given
- Day 0, 3, 7, 14, 28
- All IM in alternating deltoids
- Immunoglobulin
- 20IU/kg (adult or child)
- Infiltrated at site of wound
- if wound unclear then IM in anterolateral thigh
- never give vaccine and immunoglobulin in the same site
- Note treatment can probably wait a day following reporting (allows vaccine and immunoglobulin to be delivered)
- LITFL post by Neil Long really worth a read
- pretty common (in my quite limited experience)
- viral, mosquito borne
- one of the early presenters (incubation <1 week)
- fever, headache yadda yadda
- muscle and bone pain apparently a distinguishing feature
- low WCC and Platelets and raised LFTs
- most have the mild form
- occasional Dengue Haemorragic Fever which is the real bad boy
- Treatment – supportive
- Salmonella typhi
- incubation 1-2 weeks
- similar symptoms to malaria without the jaundice i suppose
- relative bradycardia appears to be the distinguishing feature
- Treatment
- supportive
- cipro or cefotaxime